High Palate And Tongue Tie
It's hard to adequately convey the importance of good palatal development, which begins before your baby is born. When things are working properly, your baby’s tongue molds the palate, which allows the palate to widen & broaden in utero. When things don’t work properly, a high, narrow palate results.
Tongue tie is one potential & common cause of a high-arched palate. Restricted tongue mobility, as a result of a short or tight frenulum, may change the shape of a baby's mouth and lead to a narrow or high palate.
Other causes of high palates in babies include
Congenital disorders
Genetics
Cranial Facial Differences
Poor tongue function unrelated to ties
Premature fusion of the skull bones
Excessive pacifier usage
Prolonged intubation with an endotracheal tube
Palate shape, with regards to width and overall shape, has drastically changed in the past 12,000 years. Additionally, palatal shape varies worldwide, with some ethnicities having a broader palate than others.
Compared to our ancestors, our jaws are smaller, our palates are both more narrow & higher, & as a result, we're more prone to malocclusion & teeth crowding. Poor tongue elevation due to oral dysfunction is just the icing on the cake- or possibly a byproduct of the anatomical changes through the centuries.
Types of Palates: Narrow, High-arched, & Short
A narrow palate is not necessarily the same as a high palate despite being seen together. It can be helpful to know what the differences are so you can better understand your baby's anatomy.
What is A Narrow Palate?
A narrow palate is determined to be present when the space between where your baby's first molars (and/or canine teeth) will erupt is less wide than expected. The average intermolar palatal width for a baby is ~32 mm (1.2 inches).
Ideally, your baby's palate & gum line is shaped like a wide U, rather than a skinny U or a V. A V-shaped palate occurs when the front portion of the palate is significantly more narrow (less wide) than the back portion.

Image B shows how the width of the palate is measured: Distance between C & D (where your baby’s molars will erupt. Image A shows how the depth of the palate is measured: how high the arch is compared to the top of the gums (point A). When determining if a palate is high or not, providers can make a visual assessment or feel in your baby’s mouth to determine if it’s higher than average. No rulers needed! | Photo From: Deformation of the palate in preterm infants
What is a High-arched Palate?
A high-arched palate is determined to be present when the depth of your baby's palate ( the vertical distance between the alveolar gum ridge & roof of their mouth) is larger than expected. The average palatal depth for a baby is ~10 mm (.3 inches).
There are 3 main subtypes of high palates, defined by their shape.
Channel Palate
A channel palate has a central groove in the middle of the palate, typically running the entire length of the hard palate. The central groove can range from "mild," with a decent amount of space between the sides of the channel, to severe- very little space between the sides of the channels. Channel palates are most common in babies with congenital issues or those who had prolonged intubation.
Vaulted Palate
A Vaulted (or Cathedral) Palate has a central groove in the middle of the palate, but rather than having straight angled edges like with a Channel Palate, the sides of the groove have a bit of a curve. Where as the sides of the channel palate are typically consistent, the sides of a vaulted palate become more narrow at the roof of the mouth & toward to the front, giving it a slightly more V shape. I’ve heard my friend & colleague Rachel Obrien IBCLC explain that the shape of a valuated palate is like a cross between a U & a V, which honestly is the most simple way to explain a surprisingly difficult concept.
Bubble Palate
A Bubble palate has a round depression with a pronounced rim in the middle of the palate.
It can be hard to describe palate shape, so below, you will see a few variations of high palates, including the channel Palate and bubble palate.
In most cases, the only two dimensions relevant to arches & tongue ties are width & depth, but palatal length is a third measurement that gives us insight into the shape & size of one's palate.
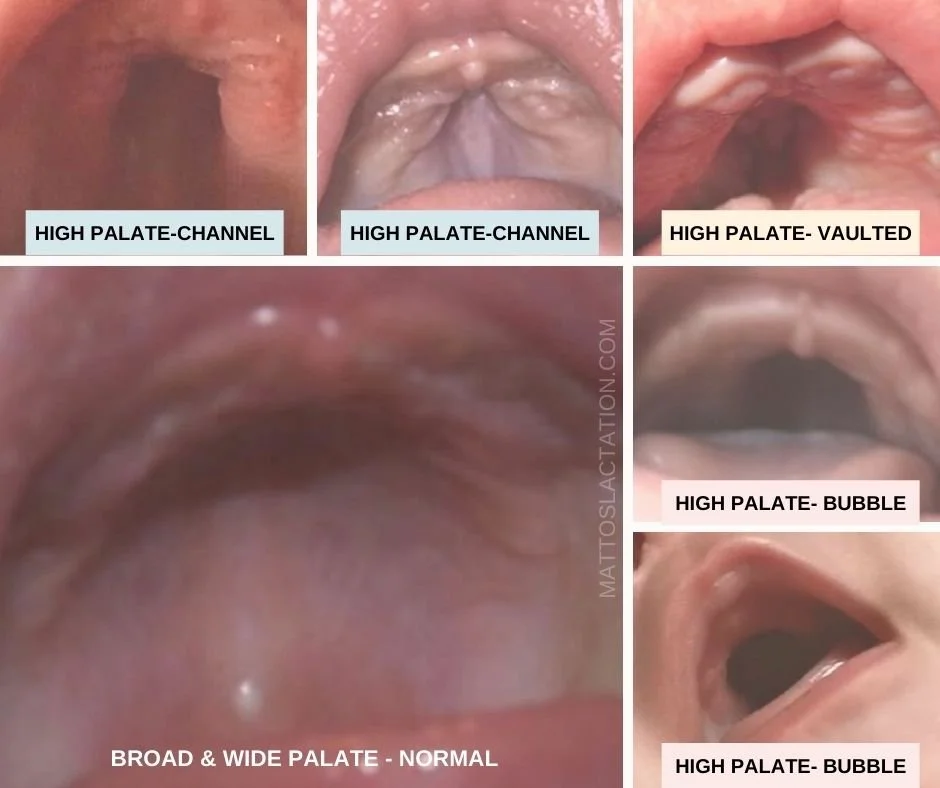
Palate shape typically does not fit neatly into any one category. The top middle picture is a great example of that. Is it a channel or a vaulted palate? An argument could be made either way. In reality, the type of high palate your baby has doesn’t matter that much. Channel, vaulted & bubble palates often leads to the same challenges & the way to resolve is universal.
What is a short Palate?
A short palate is determined to be present when the length of your baby's palate- from the gums (front) to where the soft & hard palate come together (back)- is shorter than expected. The average palatal length in babies is 1 inch. Decreased palatal length may be due to a highly arched palate, craniofacial anomaly, or genetic condition.
What kind of high palate does your baby have?
Getting photos of baby palates is surprisingly tricky. Baby's mouths are small & visualizing the hard palate can be a challenge since there is limited light in their mouth cavity. Taking a picture can help you identify which type of high palate your baby has.
Picture Taking Tip: Use a flashlight or flash on your phone when taking photos of the palate. You can look through your screen and get close to your baby's palate to take the photo. Take the picture from the same position you would properly assess for a tongue tie, with your baby's feet away from you.
Effect of A High Palate On Breastfeeding & Bottle Feeding
Some of the symptoms of tongue tie overlap or are similar to those of a high palate. It can make it challenging to determine which symptoms are due to the tie and which are due to your baby's palate.
Babies with high palates may have difficulties with breastfeeding or bottle feeding.
A high arched palate can make it difficult for babies to protect their airways during swallowing, leading to significant coughing or choking with feeds. Babies with high palates may not be able to generate enough suction to transfer milk from the breast or bottle, causing weight gain issues or weight loss.
For babies who struggle to intake enough milk to grow well with standard bottles, a special needs feeder bottle often helps. Positional changes during breastfeeding can make breastfeeding safer and more effective for most babies with high, narrow palates.
Parents breastfeeding babies with high palates often report sore/painful nipples from nursing.
High palates can cause dysfunctional feeding, resulting in nipple pain, soreness, or damage. A common culprit of nipple discomfort with breastfeeding is too shallow of a latch, resulting in the nipple being compressed against the hard palate. The pain may be quite significant with high arched palates due to the angle at which the nipple may be "folded" to reach the baby's mouth.
Babies with high palates are likely to have persistent congestion & difficulties with clearing their sinuses.
When the palate is high, the inner part of the nasal cavity is smaller than it should be. This can make breathing difficult in general, but make it near impossible to breath with any amount of congestion or inflammation in the sinuses. Babies typically have inflammation or congestion in the first few weeks, especially if they’ve received aggressive suctioning at delivery.
Babies with high palates tend to breathe through their mouths and sleep with an open mouth posture.
The relationship between open mouth breathing & palate development is complicated. A high, narrow palate can make it difficult for babies to breathe through their nose, resulting in open mouth breathing. Because nasal breathing can stimulate growth width-wise of the palate, open-mouth breathing further exacerbates the problem and prevents resolution.
One strategy to address palatal development is to encourage tongue-to-roof tongue placement during sleep using the sleepy-time posture hold, which forces nasal breathing & helps with palate expansion.
Babies with high palates often have hypersensitive, anterior gag reflexes
Tongue contact with the hard palate desensitizes the gag reflex and pushes it back to where it needs to be (near the hard & soft palate junction). When babies are unable to maintain contact with their hard palate, they may gag very easily on the breast or the bottle & their sensitive gag reflex may prevent them from getting a deep latch.
Babies with high palates may struggle with reflux or nasal regurgitation.
Clicking with feeding is a common symptom of both tongue tie & high palate. Many babies cannot elevate their tongue to create or maintain a good seal around the breast or bottle teat, and the clicking noise results from the lack of suction. Constant clicking may increase air intake during swallowing, leading to reflux. Babies tend to struggle with reflux even after a tongue tie release, due in part to their persisting high palate. Over time, as tongue function improves and the palate expands, reflux tends to get better.
Similar to reflux, nasal regurgitation may persist in tied babies, even after release, until the palate becomes more broad and wide. High palates can impact the way the nerves and muscles of the soft palate communicate, allowing for milk to enter the nasal cavity.
Unfortunately, there is not a lot of research on high palates & infant feeding, which can support my observation about reflux & nasal regurgitation. I've combined my understanding of oral anatomy, oral function, and biomechanics with my professional experience to provide the above information.
Activities To Lower Your Baby's High Palate Before & After Tongue Tie Release.
Babies' palates are pretty flexible, which is fantastic news when trying to improve feeding challenges. Flexibility may not be the best word; it doesn't mean bendable; rather, the palate easily adapts to environmental input. Thus, we can enact change on the palate by changing the inputs into the palate as the bone grows. Bone growth occurs rapidly in infants, so palatal change can happen quite quickly.
If your baby has been diagnosed with a high palate or if you suspect your baby has a high palate and are looking for at-home activities you can do to help expand your baby's palate, I highly suggest you schedule an appointment. The palate activities below should be done under the care of an oral function savvy IBCLC, as doing the activities improperly or when your baby is not ready can make feeding challenges worse.
Sleepy-Time Tongue Suction
The Sleepy-Time Suction Activity is similar to the Sleepy Time Posture Hold (video below), in that we want to encourage the tongue to suction against the palate during sleep. Unlike in the video, however, the downward pressure on the chin to break the suction is not necessary.
Anytime you notice your baby sleeping with an open mouth posture, first make sure your baby’s head is alignment with their shoulders (not tilted back or to the side). If your baby’s mouth remains open, gently press into the soft area under your baby’s chin to get their tongue to stick to the roof of their mouth.
Palate Wipers
Skip to 1:22 to view a demonstration of Palate Wipers
Palate wipers are a simple activity aimed at expanding the palate. Essentially, with your finger pad side up, you make small wiper motions from side to side. Ensure you're not pressing up into the palate but instead are just creating motion on the palate.
Palate Sweeps
Palate sweeps are a great way to apply gentle but intentional outward pressure to expand the palate. The goal with Palate sweeps is to increase the palate's width gradually. Palate sweeps are a bit more "aggressive" than palate wipers, holding outward gentle pressure for a second or two before returning to the middle to do on the other side. Because pressure, even gentle pressure, can be quite intense for babies, it can be helpful to apply slight downward pressure to the top of your baby's head during the activity.
Conclusion
High palates are another complication to an already complex situation for tongue-tied babies. Even when the ties are resolved, problems with feeding, reflux, congestion, and open mouth breathing may persist. Though things may feel (and are) complicated, overwhelming & frustrating, there are many things we can do to address your baby's feeding issues.
Luckily the management plan for high palates is similar to the plan for tongue tie; work with an oral function savvy lactation consultant (IBCLC) & get bodywork. Cranial sacral therapy can be beneficial for high palates. A tongue tie release to improve tongue mobility may or may not be necessary depending on the cause of your baby's high palate. Similarly, your baby may need to work with an OT, PT, or SLP to address the high palate factors other than oral function are contributing or if limited progress is made with an IBCLC alone.